Contact us for timely diagnosis, expert guidance, and compassionate heart care.
Rotational atherectomy, orbital atherectomy, and intravascular lithotripsy (IVL)–guided coronary angioplasty are advanced plaque-modification techniques used to treat severely calcified coronary artery disease. Under the expert care of Dr. Vinodh Kumar K, these technologies are employed to safely modify hard calcium deposits, enabling optimal stent delivery, expansion, and long-term durability.
Heavily calcified lesions pose major challenges to standard angioplasty. These advanced tools prepare the artery effectively, improving procedural success and clinical outcomes.
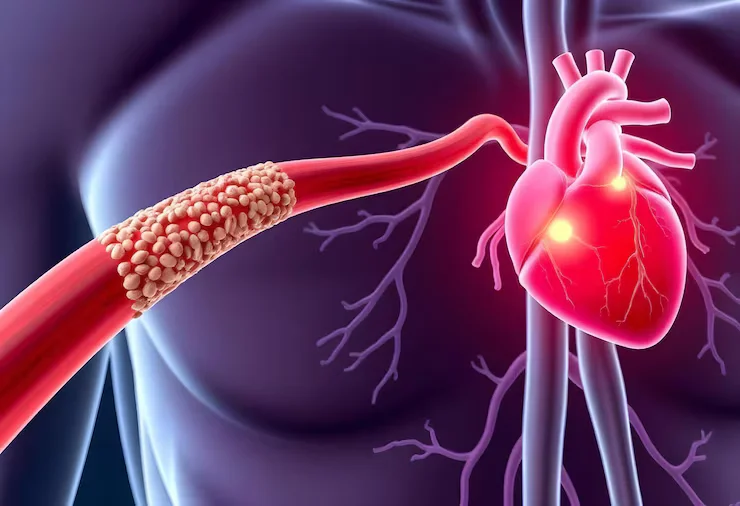
Calcification causes arteries to become rigid and resistant to balloon dilation, increasing the risk of incomplete stent expansion, restenosis, or stent thrombosis. Advanced plaque-modification techniques are essential to safely treat such lesions and restore reliable blood flow to the heart muscle.
Rotational atherectomy uses a high-speed, diamond-coated burr to selectively ablate hard calcium within the artery. This technique creates a smoother vessel lumen, allowing balloons and stents to be delivered and expanded effectively.
It is particularly useful in:
Severely calcified lesions
Long-standing, rigid blockages
Lesions resistant to balloon dilation
Orbital atherectomy employs a diamond-coated crown that orbits within the artery, modifying calcium in a controlled and uniform manner. It treats calcium circumferentially and is effective across varying vessel sizes.
This approach is beneficial for:
Diffuse and concentric calcification
Large or tapered vessels
Lesions requiring uniform plaque modification
IVL uses acoustic pressure waves—similar to kidney stone lithotripsy—to fracture deep calcium within the vessel wall while preserving soft tissue. This allows safe balloon expansion and optimal stent deployment with minimal vessel injury.
IVL is especially useful in:
Deep or nodular calcium
Calcified left main or bifurcation lesions
High-risk or fragile vessels
The primary goals of these advanced techniques are to:
Modify severe coronary calcification safely
Enable optimal stent delivery and full expansion
Reduce the risk of stent under-expansion and failure
Improve long-term vessel patency
Enhance outcomes in complex, high-risk PCI
Dr. Vinodh Kumar K selects the most appropriate modality based on lesion characteristics, vessel anatomy, and overall patient risk.
Rotational atherectomy, orbital atherectomy, or IVL may be recommended for patients with:
Heavily calcified coronary lesions
Balloon-resistant blockages
Left main coronary artery disease with calcium
Bifurcation lesions with rigid plaques
Complex or high-risk coronary anatomy
Failed previous angioplasty due to calcification
Early use of plaque-modification improves procedural success and long-term outcomes.
Care under Dr. Vinodh Kumar K involves detailed angiographic and intravascular imaging assessment (IVUS/OCT when needed) to characterize calcium depth and distribution. A tailored strategy is chosen to ensure maximum safety and effectiveness.
Post-procedure care includes optimized medical therapy, risk-factor control, and structured follow-up to maintain durable results and long-term coronary health.
Expertise in atherectomy and IVL-guided coronary interventions
Extensive experience in complex and high-risk PCI
Evidence-based selection of plaque-modification techniques
Strong focus on safety, precision, and long-term outcomes
Clear patient communication and personalized care
Access to comprehensive interventional cardiology services
Dr. Vinodh Kumar K offers advanced solutions for patients with heavily calcified coronary artery disease using rotational atherectomy, orbital atherectomy, and IVL-guided angioplasty. With expert technique and modern technology, even the most challenging coronary lesions can be treated safely and effectively.
When coronary calcium limits standard angioplasty, advanced plaque-modification restores possibilities—and blood flow.

Habitant augue molestie felis purus platea mollis mauris lectus cursus. Siverra scelerisque commodo sem nisi sed vitae in neque volutpat.